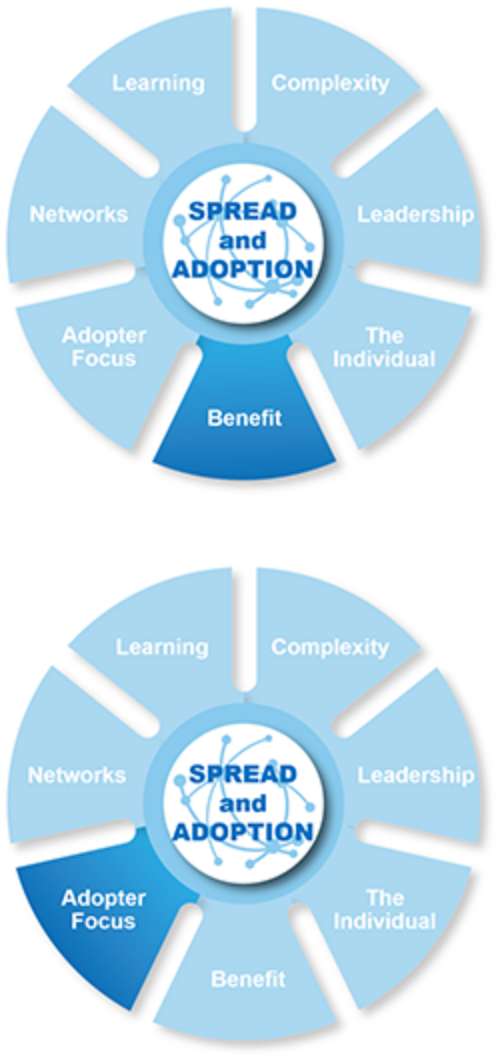
 NHS England developed a Practical Guide to support adoption. It has a mindset at its core to support the adoption of innovation in the NHS, built around seven interconnected principles. The model was been designed to support all levels of adoption – local, regional, national, and in settings where the spread and adoption of complex change is needed.
NHS England developed a Practical Guide to support adoption. It has a mindset at its core to support the adoption of innovation in the NHS, built around seven interconnected principles. The model was been designed to support all levels of adoption – local, regional, national, and in settings where the spread and adoption of complex change is needed.
This case study describes the approach taken by Health Innovation Wessex (known as Wessex Academic Health Science Network, or Wessex AHSN at the time this case study was written) took to supporting large scale adoption of FeNO testing across England through the lens of the Practical Guide. The national FeNO programme was part of the NHSEAccelerated Access Collaborative (AAC) Rapid Uptake Programme and was launched in April 2021.
FeNO tests measure the level of nitric oxide in an exhaled breath providing an indication of inflammation in the airway. Alongside a detailed clinical history and other tests, FeNO is used to support the diagnosis and management of asthma. Historically, FeNO has been widely used in secondary and tertiary care, yet there is limited adoption in primary care, presenting a large-scale adoption opportunity for the NHS to improve asthma management in primary care, and contributing to the respiratory goals outlined in the NHS Long Term Plan.
The role of Health Innovation Networks (formerly known as Academic Health Science Networks) in driving adoption
Health Innovation Wessex is one of 15 health innovation networks in England, commissioned by NHS England to support the systematic adoption of (proven) innovation. Health Innovation Wessex led the national FeNO programme, working with the national Health Innovation Network (known as the AHSN Network at the time) to enable the wide-spread adoption of FeNO testing in primary care.
Our approach to delivering the FeNO programme was described in the NHSE Practical Guide.
This case study describes our approach and provides real world examples from our experience of FeNO delivery.
 Principle 1: Complexity
Principle 1: Complexity
The model describes how complexity can exist in the innovation, the context, and the approach taken to spread and adoption.
A FeNO test is simple – it takes around 10 seconds to complete, and the result is shown on screen around 60 seconds later. Devices undertake their own quality control and do not provide a reading if a failed test has been undertaken. The value of FeNO comes from the integration of the test result into the complex asthma pathway and the value of the “So what?” question that a FeNO test result generates as part of the asthma diagnostic jigsaw – for example, are we making the right diagnosis, what is the best treatment approach? To address this complexity, the programme has always focused on the overall pathway of care and the required pathway change with FeNO integration, rather than solely focusing on the technology.
The primary care setting is most certainly complex, with 6,822 GP practices, around 1,250 emerging Primary Care Networks, many professional societies (and respiratory specific societies), NHS England and NICE to name just some of the stakeholders in care delivery. The FeNO programme aimed to gather and understand the views of as many stakeholders as possible during the programme scoping and set up phase to assess context complexity, compounded by the programme commencing during the early stages of the Covid-19 pandemic.
Deep dive – policy context
The policy context when the FeNO programme began was (and remains) complex: the NHS Long Term Plan was around a year old, Professor Sir Mike Richard’s Diagnostics: Recovery and Renewal report had been published, the NHS England national respiratory programme was describing a new direction on the back of the Long Term Plan, and Respiratory Clinical Networks were forming. In the years preceding 2020, NICE and the British Thoracic Society (BTS)/the Scottish Intercollegiate Guidelines Network (SIGN) had differing views on the role of FeNO testing but had agreed to develop collaborative clinical guidance, expected in summer 2023. The FeNO programme needed to navigate all these concurrent conversations and interactions and assess the complexity, while effectively building the case for FeNO use at scale, masterminding the programme plan, and simultaneously delivering that plan for maximum effect.
 Principle 2: Leadership
Principle 2: Leadership
Wessex AHSN took a devolved enabling leadership style to the programme, facilitating all AHSNs to work to a collective national ambition, yet supporting the implementation of FeNO testing in their local geography in their own way. We were descriptive not prescriptive in our leadership approach.
We built a collective ambition around a set of simple programme priorities and goals. We saw engagement and ambition at all scales; from individual GP practices all the way through to integrated care systems that used the resources generated by the FeNO programme to implement FeNO in the best way for their local population.
 Principle 3: The Individual
Principle 3: The Individual
At the core of the programme team were two fantastic public partners who advocated FeNO in very practical terms.
Living with severe asthma, they held the programme to account and retain its patient focus making it clear what FeNO meant to them and how it positively impacted their lives. Our public partners supported the programme and joined national events where their lived experience was regularly cited as the most powerful and motivating feature of the workshops. They were invaluable in keeping us sighted on the real world application and impact of this programme.
 Principles 4 and 5: Benefit and Adopter Focus
Principles 4 and 5: Benefit and Adopter Focus
Fundamental to our approach when spreading FeNO testing was our focus on the adopters.
Almost all the materials which comprised the FeNO implementation toolkit were designed for the adopters and were freely available to access. Many of the resources were created to be editable to allow local FeNO champions and implementation leads to adapt and use them for specific local application.
A range of people were involved in the adoption of FeNO. We extended the focus on adopters, with adoption materials supporting operational, clinical and managerial colleagues as well as directly describing the patient benefits with resources such as patient information leaflets, explanatory videos and preappointment guidance messages.
Focus on: FeNO implementation toolkit
The FeNO implementation toolkit comprised three main components:
- Information on the products
- Clinical resources (such as pathways, standard operating procedures, infection control guides and patient leaflets)
- Wider change management materials (such as project plans, training modules and case studies).
The toolkit was designed in a very practical way to support clinical and operational teams adopting and sustaining the use of FeNO testing as part of their delivery of asthma care. For example, we created a nationally-accessible accuRx message to help patients prepare for their FeNO test.
 Principle 6: Networks
Principle 6: Networks
At a national level, the connected network of AHSNs across England was core to the way we supported the adoption and spread of innovation; harnessing collective power to accelerate the pace of adoption, support sustained use and improve health outcomes.
Through quarterly FeNO Learning Collaboratives, the FeNO programme successfully connected people using FeNO, implementing FeNO and considering FeNO testing. Over 600 people attended with delegates joining from as far afield as Canada and Australia.
Wessex AHSN led and coordinated these events, but the agendas focused on the adopters and the individuals joining the collaborative to encourage them to share experiences and learning, network with other users, and generate traction and enthusiasm.
 Principle 7: Learning
Principle 7: Learning
Adopting innovation is hard, and adaptation and learning are fundamental to its success. From the outset, the FeNO programme embedded learning across three levels:
- Our national Learning Collaboratives which support people who use FeNO
- The AHSN Network community of practice which supported AHSNs directly linked with the implementation teams on the ground, and
- The National Programme Group chaired by Wessex AHSN, which took a national overview of the programme, its goals and successes.
Learning was shared across these groups and more widely with the FeNO programme’s sister programme to improve access to biological therapies for severe asthma. This relationship proved hugely beneficial as both programmes learned from each other to further improve.
At implementation level, it’s important that teams adopting FeNO tested and revised their approach to asthma care, reflected on their approaches, iterated and adapted. Our implementation toolkit included resources to enable team reflection and continuous improvement through a dedicated action learning set resource.
FeNO testing: programme outcomes
The FeNO programme gathered pace with a rapidly growing number of users across England.
Those embracing FeNO testing revamped asthma pathways, made FeNO business as usual and used FeNO testing to remove the guesswork associated with asthma diagnosis. They began to ‘think FeNO’ early: this was never done before in primary care and supported the national focus on earlier and faster diagnosis.
Supported by their local AHSN team, clinical teams used the principles described by the NHSE spread model to adopt FeNO testing in their practice. We described how the seven principles were used as part of this programme in isolation; however, the reality is - as NHSE describes – a set of ‘seven interconnected principles’ and we certainly experienced the interconnected aspects of the principles in our programme approach.
The national FeNO programme developed a suite of resources, including two training modules with free open access. Visit our Toolkits area for more details.